them bones
Osteoporosis: Prevention & REversal
Nutritional Supplements Help to Reduce and Reverse Osteoporosis & Osteopenia
by Ladd McNamara, M.D.
Discussion
 The article and protocols are for informational purposes only, and are not intended as medical advice. Please read the medical disclaimer below, and consult your personal physician prior to taking supplements and acting upon on the information presented in this article, protocol, or website.
The article and protocols are for informational purposes only, and are not intended as medical advice. Please read the medical disclaimer below, and consult your personal physician prior to taking supplements and acting upon on the information presented in this article, protocol, or website.
Osteoporosis is a chronic, potentially debilitating condition of low bone density, causing weakened bones that are susceptible to fracture. It is an under-appreciated indirect cause of death among both men and women. It is a common condition afflicting 1 in 2 women and 1 in 4 men. The good news is that it is preventable and reversible!
Impact of Osteoporosis
In the U.S. alone, there are over 1.5 million osteoporotic bone fractures per year, with over 800,000 emergency room visits and over 500,000 hospital admissions for fractures due to osteoporosis. By comparison, there are “only” 90,000 hospitalizations for breast cancer each year in the United States.
 Hip fractures are the most devastating of the fractures due to osteoporosis, accounting for over 300,000 hospitalizations per year. That number is expected to rise with the aging baby-boom generation.
Hip fractures are the most devastating of the fractures due to osteoporosis, accounting for over 300,000 hospitalizations per year. That number is expected to rise with the aging baby-boom generation.
Although few die directly from the fracture, depression and pain from immobilization has a psychological impact on both patients and their immediate family. Blood clots, thromboembolisms, and pneumonia due to immobilization are the causes of death in those suffering a hip fracture; particularly during the first 6 months after the fracture.
Shortened stature and chronic back pain are a result of compression fractures of the vertebra of the spine.
Anatomy of the Bones
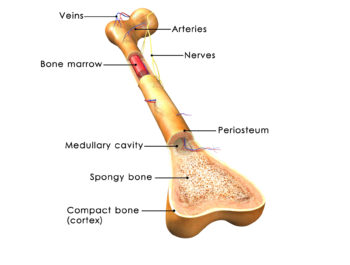 Bones are made up of living cells, collagen, and of course, minerals — mainly calcium and phosphorus. Other minerals also make up the bone, including magnesium, boron, and silicon.
Bones are made up of living cells, collagen, and of course, minerals — mainly calcium and phosphorus. Other minerals also make up the bone, including magnesium, boron, and silicon.
The bones have an outer compact cortical layer and an inner trabecular spongy area where a matrix of mineral girders are continually being created and torn down in this dynamic tissue. There is active bone turnover in which minerals are flowing in and out of the blood and into and out of the bone.
The long bones of the arms and legs have bone marrow mostly filled with fat, or yellow bone marrow, and the flat bones of the hip, sternum, shoulder blades, skull, vertebrae, and ribs have red marrow, where most of the stem cells reside, for creating both white and red blood cells.
There are two main bone cells (osteocytes) that are responsible for bone mineral turnover: osteoblasts that lay down minerals (mostly calcium and phosphorus) and osteoclasts that resorb minerals and release them into the bloodstream. Various hormones influence these cells; and the balance of hormones, available micronutrients, physical strain on the bones, and other factors signal the activity of one or the other osteocytes to carry out their function.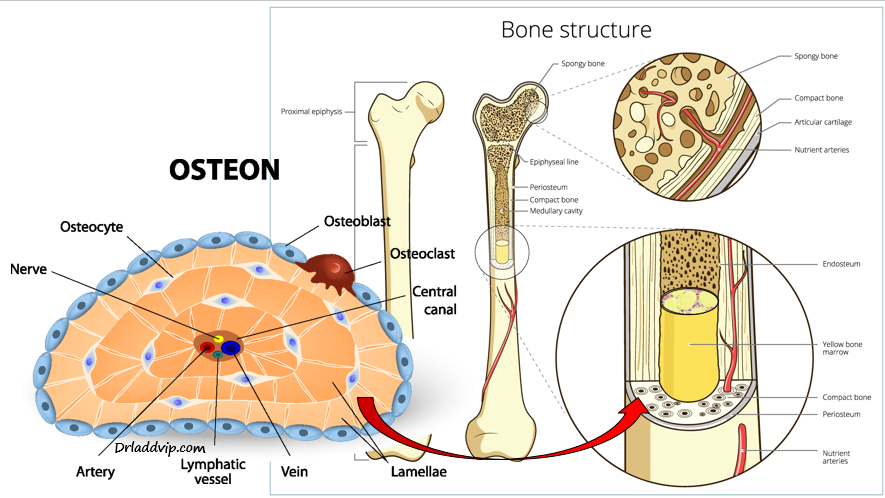
In a perfect situation, the amount of bone being laid down and the amount of bone being resorbed would be equal in a steady state. However, as we age, there is a slowing down of osteoblastic activity, likely due to the wearing out of the cell’s mitochondria, and/or vitamin and mineral deficiencies, resulting in a one percent loss of bone density per year in both men and women.
However, as both estrogen and testosterone decline as women approach menopause, the rate of bone density loss increases to 2 – 3 percent each year, putting a woman at a significant risk for osteoporosis, particularly if she started out with low bone density from her teenage years when peak bone density is established.
Importance of Supplementation in Adolescence
Once a person’s peak bone density is established, the bones do not get any stronger than their set point. I often diagnosed patients between ages 50 – 55 with osteoporosis at their first screening bone density scan. They would express surprise that menopause had “so soon” had the effect of producing osteoporosis. We worked to strengthen their bones with micronutrient supplementation (as in my protocol below), hormone replacement (unless contra-indicated), and medications for the more severe cases.
I informed my patients that they probably never had developed optimal bone density during puberty and therefore had spent most of their adult lives with less than strong bones. With the loss of bone density each year as one ages, and the increased rate of bone loss near menopause, it was enough to result in full-blown osteoporosis. Although we were able to get their bones stronger over the course of one to two years, we would only be able to get them to the density they had at age 35 – 40, which still may have been mildly osteoporotic, i.e., having osteopenia.
The determinants of bone density for both young men and women occur during puberty, with a confluence of factors, including genetics, hormones, micronutrient supplementation, a healthy diet, an active lifestyle, and avoidance of toxic chemicals in the food, drinks, water, and the environment. Some medications can have a detrimental influence as well, particularly corticosteroids.
By the time a person is 18 – 20 years old peak bone density is set. This is why I encourage parents and grandparents to make sure teenagers are getting proper supplementation with quality nutritional supplements, reducing the amount of soda, especially caffeinated drinks, eating healthy, and keeping physically active.
Risk Factors of Osteoporosis
• Age
• Gender (women > men)
• Peak Bone Density Established in Puberty
• Menopause (without hormone replacement)
• Inactivity
• Inadequate Intake of Micronutrients (vitamins and minerals)
• Race (Caucasians and Asians > Blacks)
• Low Body Weight (< 125 lbs, and BMI < 21 is at increased risk)
• Chronic Disease
• Corticosteroid Medications
• Smoking
• Alcohol
• Caffeine (sodas, coffee, tea)
Medications for Treating/Reversing Osteoporosis
Although there are medications that are used to treat osteoporosis, there are side-effects, some of them quite serious; including jawbone osteonecrosis and blood clot formation, depending upon which medication is being used. However, when the risk of fracture is high, as with severe osteoarthritis, it would be wise to be on the medications, at least until the severity of the disease is lessened to the point of mild osteoporosis or better.
All medications should be used in conjunction with the all-important vitamins and minerals, especially calcium, magnesium, boron, silicon, vitamin D3, and grape seed extract. Grape seed extract, combined with vitamin C, helps with collagen and elastin formation in the bone, to allow for some flexibility. Without flexibility, mineralization can occur rapidly with medications, but the bones will be brittle and at risk of fracture!
Medications such as Fosamax, Actonel, Boniva, Forteo, and Evista help strengthen bones and reduce fractures by inhibiting osteoclastic mineral absorption of bones, allowing the osteoblasts a chance to be more active relative to the osteoclasts.
Soy Isoflavones
 Soy isoflavones stimulate estrogen receptors in the bone, reducing the loss of whole body bone mineralization. (1) Although soy isoflavones cannot be used to replace the powerful effects of estrogen and testosterone replacement on bone, they can be used in conjunction with other micronutrients for slowing bone loss.
Soy isoflavones stimulate estrogen receptors in the bone, reducing the loss of whole body bone mineralization. (1) Although soy isoflavones cannot be used to replace the powerful effects of estrogen and testosterone replacement on bone, they can be used in conjunction with other micronutrients for slowing bone loss.
In addition, soy isoflavones are beneficial to both men and women, especially in those taking hormone replacement, as soy isoflavones effectively ‘block’ estrogen from connecting to estrogen receptors on the breasts and prostate. Although there is yet to be proof that soy isoflavones reduce the risk of breast cancer, there are enough scientific studies to show that soy isoflavones do not increase the risk of breast cancer. A woman can get the bone and heart benefits of soy isoflavones, and also the theoretical benefits to the breasts without concern for increasing her risk of breast cancer.
Beta Glucans
 Beta glucans have been shown to enhance the maturation and activity of osteoblasts, and inhibit the maturation and activity of osteoclasts, thereby resulting in the net effect of promoting bone mineralization. (2, 3)
Beta glucans have been shown to enhance the maturation and activity of osteoblasts, and inhibit the maturation and activity of osteoclasts, thereby resulting in the net effect of promoting bone mineralization. (2, 3)
Beta glucans are polysaccharide fiber micronutrients that are derived from the cell membranes of the Reishi and Shiitake mushrooms, as well as baker’s yeast extract. Beta glucans have been used for years in Chinese medicine as immune modulators, and cancer fighters. And as has been discovered over the past few years, they can be used with the other micronutrients to help prevent and reverse osteoporosis.
Vitamin K2
Vitamin K2 activates the calcium-binding actions of two proteins — matrix GLA protein and osteocalcin, which help to build and maintain bones. Vitamin K2 actively removes calcium from arteries, reducing arterial plaque and reducing the risk of heart disease, and helps place it into bones, to reduce the risk of osteoporosis and bone fractures. (4 – 7)
Vitamin K2 as MK-4 is the most active in inducing these proteins to increase bone density, but supplementation with MK-4 has very little bio-availability, since it is mostly cleared from the blood quickly (within 8 hours). Supplementation with MK-7 seems to be the preferred formulation, since the blood levels remain elevated for greater than 24 hours, and MK-7 is converted into MK-4 within the body.
A person with osteoporosis should consider supplementing with at least 450 mcg per day of vitamin K2 (MK-7), along with 8,000 – 10,000 IU of vitamin D3.
Conclusion
Osteoporosis is an under-appreciated chronic debilitating disorder, with potentially fatal consequences. Prevention starts in puberty with adequate nutritional supplementation that should be continued throughout one’s lifetime. Reducing the risk factors that are in one’s control and increasing weight-bearing exercises, such as walking, jogging, and mild weight-lifting at least 3 times per week are enough to prevent and reverse this disease.
Supplement Protocol for Osteoporosis
Please read the above article in detail to know that it is not just nutritional supplements that are required to prevent and reverse osteoporosis, but a combination of many factors. Sometimes medications are necessary for reversing osteoporosis; but they should always be taken in conjunction with proper nutritional supplementation.
High doses (>1000 IU) of vitamin D should not be taken without also supplementing with vitamin K2 (MK-7). For every 1000 IU of vitamin D3, one should consider taking 45 mcg of vitamin K2. For example, if you take 4000 IU of vitamin D3 per day, seriously consider taking at least 180 mcg of vitamin K2. If you take 10,000 IU of vitamin D3 per day, consider taking at least 450 mcg per day.
The article and protocols are for informational purposes only, and are not intended as medical advice. Please read the medical disclaimer below, and consult your personal physician prior to taking supplements and acting upon on the information presented in this article, protocol, or website.
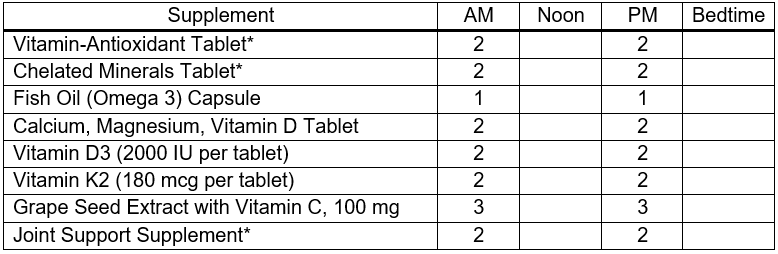
Minimal Protocol for Osteoporosis & Osteopenia
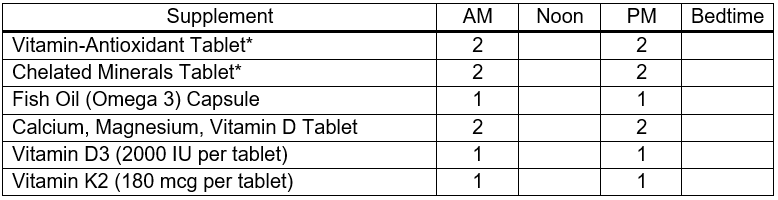
Basic Protocol for Osteoporosis & Osteopenia
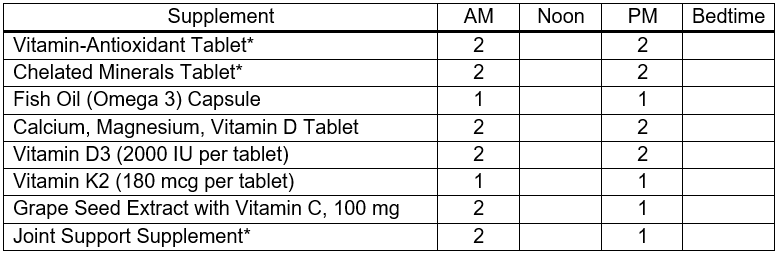
Average Protocol for Osteoporosis & Osteopenia
Advanced Protocol for Osteoporosis & Osteopenia
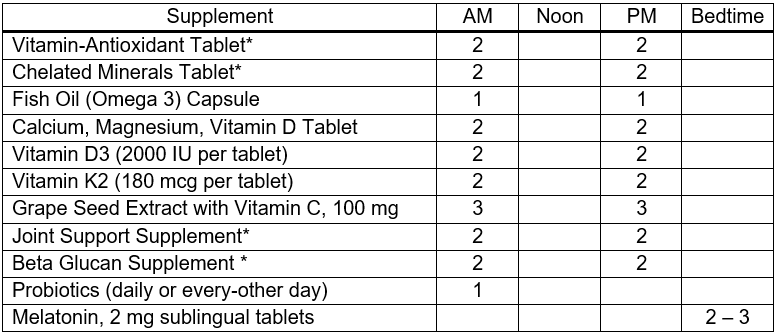
- AM: With, or after breakfast
- Noon: At lunchtime with food, or shortly thereafter
- PM: Late afternoon with food, or at, or after dinner
- Please see my list of ingredients (below) that I like to see provided by a foundational vitamin and mineral supplement.
- Vitamin K2 is usually found in a foundational multi-mineral supplement, and it is also provided as a stand-alone product, usually as 180 mcg tablet. Taking at least one per day is for preventative use; that is to prevent cardiovascular disease, and osteoporosis, as well as to help prevent BPH, along with other micronutrients. When BPH is present, consider 360 to 1,800 mcg per day of vitamin K2. There is no known toxic dose; and it also has benefits for the arteries and bones.
- Joint Support Supplement providing glucosamine and Meriva brand curcumin, among other micronutrients.
- Beta Glucan Supplement, derived from extracts of reishi and shiitake mushrooms, as well as baker’s yeast extract. This is a powerful immune support supplement, giving it anticancer effects, as well as bone support.
Ingredients that I like to see provided collectively by vitamin-antioxidant & chelated mineral tablets
Vitamin A, mostly as Beta Carotene
Vitamin C
Vitamin D3
Vitamin E
Vitamin K (K1 & K2)
B-Complex Vitamins
Curcumin (turmeric extract)
Quercetin
Green Tea Extract
Olive Extract
Rutin
Resveratrol
Choline
Lutein
Lycopene
N-Acetyl-L-Cysteine (NAC)
Calcium
Magnesium
Iodine (as potassium iodide)
Zinc
Selenium
Copper
Manganese
Chromium
Molybdenum
Including Ultra Trace Minerals
Medical Disclaimer:
Information on this website, written, spoken, or in any other communication by Dr. Ladd McNamara or any other information or reference is for informational purposes only. The information provided on this website is a result of years of practice, experience, and study by the author. This information is not intended as a substitute for the advice provided by someone’s personal licensed physician or other healthcare professional, or any information contained on or in any product label or packaging. Do not use the information on this website, or any other form of communication from Dr. Ladd McNamara or the Dr. Ladd VIP Program, for diagnosing or treatment of a health issue or disease, or for the prescribing of medication or the use of supplementation without a discussion with your licensed health professional first. At best, the information provided on this website is only meant to supplement information provided by your own doctor or health professional, not to replace medical advice. The information from this website is not meant to cover all possible uses, precautions, interactions or possible adverse effects of nutritional supplements with or without medications, or in conjunction with specific medical conditions. The information from this website may not fit your specific health circumstances. Never delay seeking medical care or disregard advice from your health care professional because of information you have received directly or indirectly from this website, from the Dr. Ladd VIP Program, or from Dr. Ladd McNamara himself. Always speak with your physician or other healthcare professional before making any changes to your medication or embarking on a nutritional, herbal or homeopathic supplement program, or before using any treatment for a health concern. If you have, or suspect that you have, a medical problem, contact your health care provider promptly. Do not disregard professional medical advice or delay in seeking professional advice because of something you have read or heard on this website, or due to any other information from Dr. Ladd McNamara or his representatives. Information provided on this website or the V.I.P. Program, and the use of any products or services mentioned on this website (or as a result of information provided this program, article, or website) by you DOES NOT create a doctor-patient relationship between you and Ladd McNamara, M.D. Information and statements regarding dietary supplements have not been evaluated by the Food and Drug Administration and are not intended to diagnose, treat, cure, or prevent any disease.
References
- Wong WW, et al. Soy isoflavone supplementation and bone mineral density in menopausal women: a 2-y multicenter clinical trial. Am J Clin Nutr. 2009 Nov;90(5):1433-9.
- Przekora A, Ginalska G. Enhanced differentiation of osteoblastic cells on novel chitosan/β-1,3-glucan/bioceramic scaffolds for bone tissue regeneration. Biomed Mater. 2015 Jan 13;10(1):015009.
- Przekora A, Ginalska G. Addition of 1,3-β-D-glucan to chitosan-based composites enhances osteoblast adhesion, growth, and proliferation. Int J Biol Macromol. 2014 Sep;70:474-81.
- Shearer MJ, et al. Vitamin K nutrition, metabolism, and requirements: current concepts and future research. Adv Nutr. 2012 Mar 1;3(2):182-95.
- Myneni VD, Mezey E. Regulation of bone remodeling by vitamin K2. Oral Dis. 2017 Nov;23(8):1021-1028.
- Rønn SH, et al. Vitamin K2 (menaquinone-7) prevents age-related deterioration of trabecular bone microarchitecture at the tibia in postmenopausal women. Eur J Endocrinol. 2016 Dec;175(6):541-549.
- K Giri T, et al. Maximal dose-response of vitamin-K2 (menaquinone-4) on undercarboxylated osteocalcin in women with osteoporosis. Int J Vitam Nutr Res. 2019 Feb 28:1-7.
All materials on this website, written, audio, visual, are copyrighted by Ladd McNamara, Inc., and are not to be distributed, duplicated, shared, posted to another website or social media sites (including Facebook, etc.), except for under the Terms of Use for sharing approved articles and videos.
As a VIP member, you agree that you will NOT share any written, audio, video, or any other proprietary materials from this website with those in your organization, other associates, or team members; and that you will only share approved articles/protocols and videos with your OWN PERSONAL & IMMEDIATE customers, clients, and prospective customers/clients. Doing so, would result in the loss of your Dr. Ladd VIP membership without a refund.
Thank you for your honesty and integrity.
About the Dr. Ladd VIP Program
There are many more articles on various subjects, as well as videos on health concerns, along with specific nutritional supplement protocols for managing health concerns and disease. Of course, this is all for informational purposes, and not to be taken as medical advice. (See medical disclaimer above.) Please learn more at www.drladdvip.com.
Please read about the benefits of being a Dr. Ladd VIP Member. It is a subscription-based personal program to better your health, energy, and passion for life, and for helping others. This program includes on-going support for yourself, and as you help customers and clients with your health enterprise.
Do you have a need to understand how NUTRITIONAL SUPPLEMENTS can benefit the health of people suffering from any number of chronic diseases; such as Heart Disease, Cancer, Diabetes, Arthritis, Dementia, Lyme Disease, Autoimmune Diseases, and Many More!
- Do you have a need for SUPPLEMENT PROTOCOLS as to what specific supplement combinations to use?
- How about WHY SUPPLEMENTS? How do you chose a QUALITY BRAND?
- Do you have a need to BETTER ASSIST CUSTOMERS in making a good decision?
- How about ON-GOING SUPPORT for ON-GOING QUESTIONS?
- How about YOUR PERSONAL HEALTH, and/or Your PERSONAL RELATIONSHIPS?
Happiness and Health includes not only being free of disease, but passionately engaged in a relationship, in life, and in helping others! It means living with less stress, more fun, and activity.
The Dr. Ladd VIP Program is about Vitality, Intimacy, and Passion, being balanced in all aspects of life, and helping others to get there too.
 Please read more at www.drladdvip.com, and take advantage of the Video Courses, the Supplement Protocols, Articles, Downloadable PDFs, and Dr. Ladd VIP Facebook Community and Support. “Have me in your back pocket” by becoming a VIP Member Today!
Please read more at www.drladdvip.com, and take advantage of the Video Courses, the Supplement Protocols, Articles, Downloadable PDFs, and Dr. Ladd VIP Facebook Community and Support. “Have me in your back pocket” by becoming a VIP Member Today!
If you are not a VIP member, please subscribe to my email list. If you are already a VIP member, no need to subscribe to the email newsletter list. Thank you.
dr. ladd
Please learn more about the Dr. Ladd VIP program here: www.drladdvip.com.
Please Subscribe to Dr. Ladd’s Email List
Receive health and website updates, as well as information on upcoming FREE health-related webinars.
All information, written or video, is copyrighted by Ladd McNamara, Inc., and is not to be shared, duplicated, or posted to other websites or social media platforms without express permissin from Ladd McNamara, M.D. Thank you.
Dr. Ladd’s V.I.P. Program and Website is Owned and Operated by Ladd R. McNamara, M.D. and Ladd McNamara, Inc., a California corporation.